The CMS ACCESS Model Is an Operations Contract. Here's the Math.
CMS's ACCESS Model pays as little as $144 of a $180 allowed amount per behavioral health patient per year, half of it withheld, with a 25% penalty for network leakage. An operator's guide to the math, the three problems that decide your payout, and why the pioneers still win.
The CMS Innovation Center's ACCESS Model (Advancing Chronic Care with Effective, Scalable Solutions) is a 10-year program that pays for technology-supported chronic care in Original Medicare across four tracks: behavioral health, MSK, CKM, and eCKM. It launches July 5, 2026, and CMS maintains a live list of accepted participants here.
Everyone has read the program summaries. Far fewer people have sat with the payment mechanics. We have, because our customers run clinical operations for a living, and ACCESS is the most operationally demanding payment model CMS has ever shipped. Here is the picture from the operator's seat.
The economics force radical operational efficiency
Take one behavioral health patient. The allowed amount is $180 a year, which blends Medicare's 80 percent with the patient's 20 percent coinsurance. Waive the coinsurance, as most participants plan to, and you keep the Medicare share: $144 a year.
Half of that, $72, is paid out monthly across the year, about $6 a patient a month you can count on. The other $72 is withheld until the end of the 12-month period, and you only collect it in full if your panel clears two thresholds.
There is no pricing lever in this program. The rate is the rate. The only lever you control is cost, which means the participants who win are the ones who run the leanest operation, not the ones with the best pitch deck.
The three problems that decide your payout
Problem one: patients leak out and trigger the Substitute Spend penalty. If a patient can't get an appointment in your network fast enough, they see an outside fee-for-service provider for the same condition. CMS tracks this. Fall below a 90% in-network rate and you lose up to 25% of your payments. The threshold leaves almost no slack: a handful of patients booking a new PT eval or therapy intake elsewhere is enough. Every unfilled appointment slot is a patient one phone call away from triggering your Substitute Spend penalty.
Problem two: the withheld 50% only pays out if patients complete 12 months. Full payment requires at least half your panel to finish their full 12-month period and hit every outcome target. That means every patient stays on schedule for check-ins, PROM collection windows, and reading cadences, all year, documented to audit fidelity. One slipped cadence is a patient who can't count toward your attainment rate. This makes outcome-cadence operations a cash flow gate, not a clinical nicety.
Problem three: the $144 ceiling means admin cost decides profit. If schedulers, credentialing coordinators, and payroll reconciliation cost you $200 per patient per year in loaded labor, the model is dead before your first reconciliation. The cost to serve an ACCESS patient has to approach zero marginal admin labor. There is no other way the math closes.
This is the math that moves scheduling automation and demand forecasting from nice-to-have to survival. It is also, candidly, what we build. Our platform takes roughly 74% of back-office workload and about 90% of scheduler time off the table. Under most contracts those numbers are an ROI story. Under ACCESS they are the difference between a viable line of business and an unviable one.
So why participate at all? Because the pioneers get paid later.
Three reasons the companies on this list are smarter than the rates suggest.
The commercial payers are coming. Fourteen major payers, including UnitedHealth Group, CVS, Cigna, Humana, and a long list of Blues, have committed to launching ACCESS-style programs for their own populations targeting January 1, 2028. Commercial rates historically run a multiple of Medicare. The 2026 and 2027 performance periods are a paid dress rehearsal for the real market.
CMS publishes everyone's results. Your outcome attainment rate will be public. When commercial payers choose partners for 2028, they will pick from a public leaderboard of who already proved they can run this model. Two years of published outcomes is a credential no late entrant can buy.
The bar rises. The Year 1 outcome threshold is set at 50%, and CMS has signaled it will increase. The earliest entrants get graded on the easiest curve.
The participants who do this well will not make their money on Medicare ACCESS. They will make it on everything ACCESS unlocks.
Protecting the 25%: fill rate is the whole game
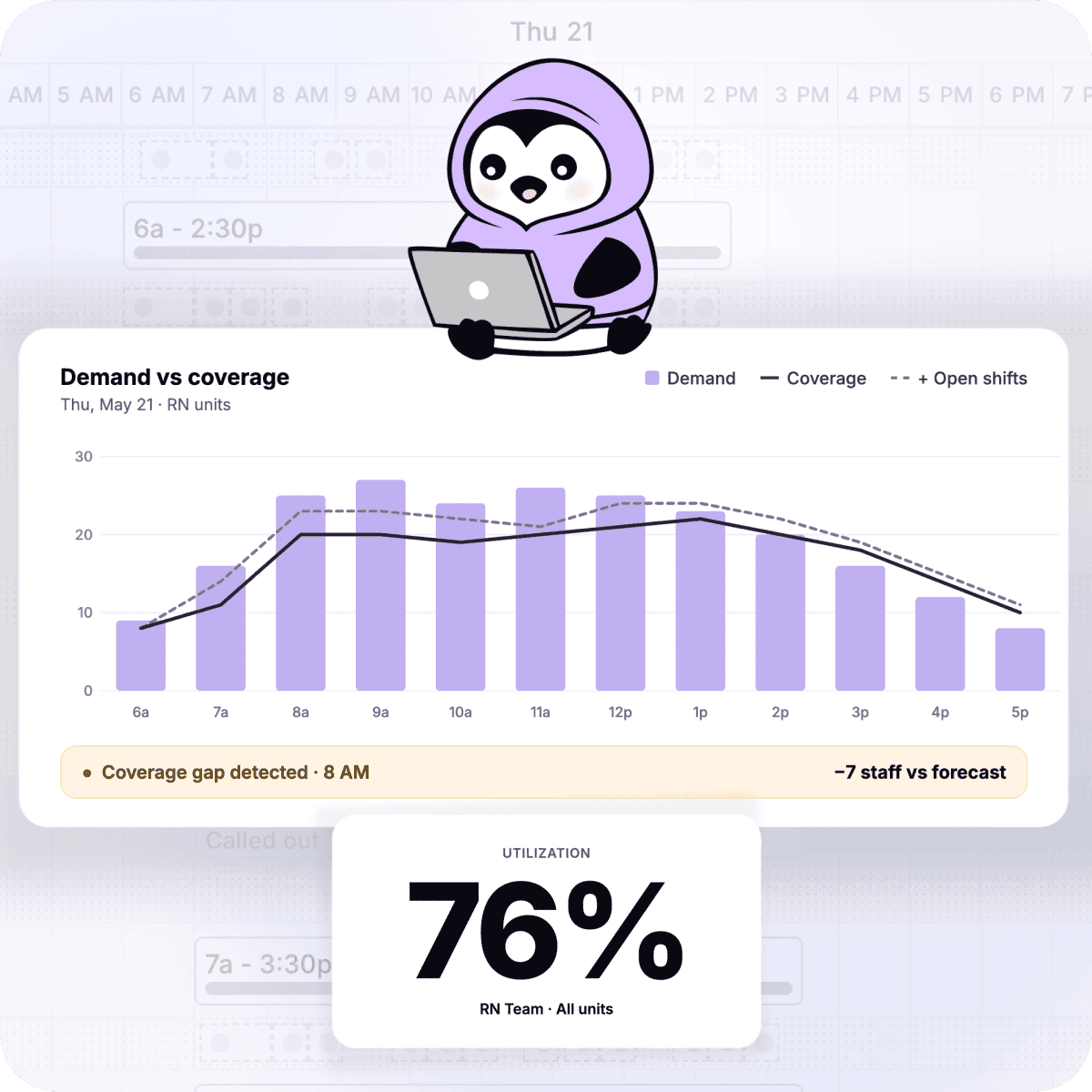
The Substitute Spend penalty is mitigated by exactly two capabilities: demand forecasting that tells you how much provider capacity you need before you need it, and provider availability orchestration that makes sure the capacity is actually bookable when the patient calls. Patients book in-network when in-network is the easy option. They leak when it isn't. This is a solvable problem, and it is the one we solve every day.
If you're on the list, or applying for the January 2027 start
We run scheduling and capacity operations for telehealth networks and hospitals. We've cut clinics' scheduler workload by about 90% and back-office operations by 74% on the platform.
Here is the hypothesis we'd put in front of any participant: with the Substitute Spend rule, any patient who can't book with you fast enough and sees another Medicare provider costs you up to 25% of payments, against a maximum of $144 per patient. Getting your coverage model right before July is not optional.
If you're planning for July, we'd love to trade notes on how you're approaching ACCESS. Book some time with our team.
Congratulations to the participants
A few of the accepted participants we're rooting for:
Headspace · Mederva Health · Headway · SonderMind · Concert Health · TailorCare · Bold · PocketRN · Wysa · Limbic · Innerwell · Override · Holon Health · Plethy · JOGO Health
The full, continuously updated list is on CMS's site. CMS is reviewing applications on a rolling basis; applications after May 15, 2026 are considered for a January 1, 2027 start.
For the full payment schedule, the clinical targets, and the operational requirements broken down track by track, see the follow-up to this post, “The ACCESS Model, Fully Priced.”
The information in this post was accurate as of Q1 2026.